Category: Medical
Addressing Rotator Cuff Tears through Arthroscopic Surgery

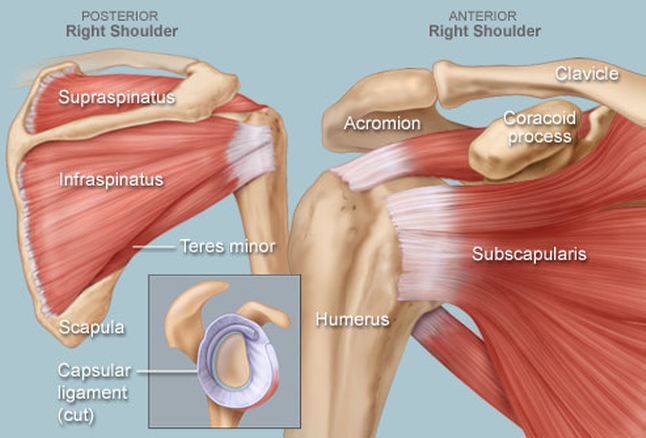
Rotator Cuff Tears
Image: orthoinfo.aaos.org
An established presence in the Milwaukee medical community, Dr. Mark Wichman practices with Aurora Advanced Healthcare Orthopaedics. Dr. Mark Wichman’s areas of focus include arthroscopic surgery of the shoulder, and he has extensive knowledge of shoulder stabilization and rotator cuff repair techniques.
Complete tears to the rotator cuff typically require reattachment of the tendon to the head of the upper arm bone (humerus). In less serious cases, a debridement, or smoothing and trimming procedure, may be undertaken.
The arthroscopic approach to surgery is less invasive than traditional open incisions, which may still be required in complex and large-tear cases. With arthroscopy, a tiny camera is inserted into the shoulder joint, with the moving images generated utilized in guiding extremely thin instruments that address the problem. This approach requires only small incisions and can usually completed in a day as an outpatient procedure.
Following surgery, a sling is employed to immobilize the arm, with the shoulder typically requiring between four to six weeks of healing to reach a point where normal movement outside of a sling is recommended.
Joints of the Shoulder

Management of the Unstable Shoulder: Arthroscopic and Open Repair
Image: amazon.com
As an orthopaedic surgeon with Aurora Advanced Orthopaedics in Milwaukee, Wisconsin, Dr. Mark Wichman draws on particular experience in shoulder stabilization. Dr. Mark Wichman has taught on this subject at the American Academy of Orthopaedic Surgeons’ annual meeting and is a chapter author for the book, Management of the Unstable Shoulder: Arthroscopic and Open Repair.
The shoulder mechanism exists at the intersection of the humerus, the clavicle, and the scapula. The articulation among these three bones, which also connect with the ribs and spine, form the joints of the shoulder.
The glenohumeral joint presents where the head of the humerus, or upper arm bone, fits within a concave depression of the humerus, or shoulder blade. This articulation forms a ball-and-socket interface. This is the main location of a shoulder dislocation, where the ball of the humerus pops out of its articulation with the glenoid socket of the scapula.
There are also smaller joints, with less range of motion, in places where the clavicle articulates with the scapula and sternum. The sternum, or breastbone, meets the clavicle at the sternoclavicular joint, located at the base of the neck. The more distal end of the clavicle, meanwhile, meets a bony projection of the sternum known as the acromion at the acromioclavicular (AC) joint. It is trauma at this joint that is referred to as a shoulder separation.
The fourth joint of the shoulder lies at the back of the body, where the scapula articulates with the ribs. This is known as the scapulothoracic joint and is not always included in the category of shoulder joints, though it does involve the motion of the shoulder blade.
Common Acute Injuries to the Knee

Acute Injuries to the Knee
Image: webmd.com
For more than 20 years, Dr. Mark Wichman has served as an orthopaedic surgeon with Aurora Advanced Orthopaedics in Milwaukee, Wisconsin. In that role, Dr. Mark Wichman has treated numerous acute knee injuries.
Acute injuries, which occur as a result of impact or other sudden trauma as opposed to overuse, can damage any number of the soft tissues of the knee. The anterior cruciate ligament (ACL) is subject to tearing upon a poor jump landing or rapid direction change, while the posterior cruciate ligament (PCL) may tear upon impact to the kneecap. Tears in either ligament can interfere with the front-to-back stability of the joint.
The medial collateral ligament (MCL), which runs along the side of the knee, is an even more commonly injured structure. Tears to this ligament occur when an impact to the outside of the knee pushes the joint inward, while a blow that sends the knee outward can injure the lateral cruciate ligament (LCL) on the knee’s interior side.
Other vulnerable structures in the knee include the patellar and quadriceps tendons, which connect the leg bones to the joint. These commonly occur due to falls, improper jump landings, or impact, and are most prevalent among athletes of middle age.
Injuries to the meniscus, a cushion of cartilage inside the knee joint, may also be more likely as the athlete ages. Like the ACL, these tears can occur when the individual twists, turns, or changes direction rapidly, though the kind of sudden movements that cause tearing may be much more subtle in an older individual.
Meniscus Transplant Surgery

Meniscus Transplant Surgery
Image: verywell.com
Dr. Mark Wichman is a Milwaukee-based orthopedic surgeon with Aurora Advanced Healthcare Orthopedics. With over 20 years of experience, Dr. Mark Wichman applies his expertise to a number of conditions, including injuries and degenerative conditions of the knee, shoulder, ankle, and elbow. Physicians at Aurora Advanced Healthcare Orthopedics performed the first cartilage transplant in 1997.
The meniscus is a C-shaped piece of cartilage that provides cushioning and shock absorption for the knee joint. When that cushioning is damaged or worn, significant paint and arthritis can develop. A patient will often undergo arthroscopic surgery to have the meniscus trimmed or repaired. If the patient meets certain criteria, he or she may be a candidate for a meniscus transplant.
During a meniscus transplant procedure, the damaged tissue is replaced with donor cartilage that has undergone extensive testing. After the surgery, a patient should expect to immobilize his knee for 4-6 weeks. Then, he will undergo several weeks of physical therapy. Normal daily activities can be resumed after two to three months. The risk of complications from a meniscus transplant are very small.
A patient is a candidate for a meniscus transplant if he is missing over half of a meniscus, is under 55 year’s old, healthy, active, and exhibits normal alignment. He must also show evidence of very little arthritis and damage to articular cartilage.
Shoulder Dislocation vs. Separation
Shoulder
Image: webmd.com
Dr. Mark Wichman, an orthopedic surgeon with Aurora Healthcare, has practiced in his specialty for more than 25 years. Particularly experienced in the treatment of shoulder instability, Dr. Mark Wichman stands out as author of a chapter on interval and posterior plication in the textbook Management of the Unstable Shoulder.
Typically, patients with shoulder instability have either a dislocation of the glenohumeral (GH) joint or a separation of the acromioclavicular (AC) joint. Separation of the AC joint indicates damage to the ligaments connecting the collarbone to the upper scapula. Because these ligaments play a crucial role in suspension of the arm, the humeral bone can then slip out of place and push toward the tip of the shoulder.
A dislocation of the GH joint, by contrast, occurs when the humerus slips out of the cup formed by the glenoid structure of the scapula. It indicates a weakness in the connection between these neighboring structures, most often exacerbated by a traumatic injury. Dislocation typically manifests as an anterior shift of the humeral head, though some patients experience a posterior shift or a universal looseness throughout the joint.
Either condition may potentially be treatable through surgery, though any decisions regarding intervention will depend on the patient’s condition. Areas of consideration include the patient’s age and activity level, as well as the severity and frequency of separation or dislocation.
Dr. Wichman has been team physician for the Milwaukee Admiral’s hockey team for 13 years. Shoulder dislocations and separations are extremely common among professional hockey players. Arthroscopic techniques for repairing dislocated shoulders and separated shoulders have come a long way allowing these techniques to help professional athlete and weekend athletes alike.
Arthroscopic Repair of Anterior Cruciate Ligament Tears

Anterior Cruciate Ligament Tears
Image: orthoinfo.aaos.org
Dr. Mark Wichman, an orthopaedic surgeon at Aurora Advanced Orthopaedics, has more than 25 years of experience in practice. Particularly expert in knee and shoulder repair, Dr. Mark Wichman focuses on the use of arthroscopic techniques.
In the human knee, four primary ligaments serve as connectors between the femur bone of the thigh and the tibia bone of the shin. The anterior cruciate ligament, or ACL, runs diagonally across the middle of the knee. Responsible for keeping the tibia behind the femur, it also provides rotational stability.
Although partial tears of the ACL may respond to nonsurgical interventions, complete tears most often require surgical reconstruction. For this, physicians typically prefer utilizing arthroscopic techniques, which involve the use of specialized instrumentation and surgical cameras that fit through small incisions in the skin and are minimally invasive.
To perform such a procedure, a surgeon will take a graft from either the patient’s own hamstring or patellar tendons or from a cadaver donor. The surgeon then adjusts the harvested tendon to the correct size. After removing the damaged ACL and any nearby debris, the surgeon introduces the graft and connects it to the tibia.
The surgeon then repairs any secondary damage and closes the site. As time goes on, new bone grows at the site where the graft is attached, thus increasing the stability of the new ACL.
Anatomy of the Shoulder
Shoulder
Image: webmd.com
Dr. Mark Wichman, a board-certified orthopedic surgeon, has practiced in the city of Milwaukee for more than 20 years. Part of Aurora Advanced Orthopaedics since 2009, Dr. Mark Wichman focuses on minimally invasive procedures for the knee and shoulder.
The shoulder joint is one of the largest and most mobile in the human body. It is formed at the point at which the humerus of the upper arm rests like a ball inside the socket of the shoulder blade, or scapula. A part of the larger shoulder joint, the structure created by the scapula and humerus is known as the glenohumeral joint.
The shoulder region also contains the coracoid process and acromion, both of which are bony projections of the shoulder blade. The acromion comes into contact with the clavicle, or collarbone, at the acromioclavicular joint. Meanwhile, the clavical contacts the sternum at the sternoclavicular joint, which facilitates movement of the collarbone.
Each of these joints also features a network of muscles, tissue, and cartilage. The rotator cuff surrounds the full shoulder to offer support and range of motion. A fluid sac known as the bursa protects the rotator cuff, and the cartilage of the labrum cushions the humerus as it moves in the shoulder joint.
American Academy of Orthopedic Surgery Backs Medical Liability Reform

American Academy of Orthopaedic Surgery
Image: aaos.org
Dr. Mark Wichman earned both a bachelor of science and his doctor of medicine from the University of Wisconsin in Madison. Since 2009, Dr. Mark Wichman has served as an orthopedic surgeon at Aurora Advanced Healthcare in Milwaukee. He belongs to the American Academy of Orthopedic Surgery (AAOS).
One the major focuses of the AAOS is reform of the medical liability system in order to improve overall patient care. The current system of liability is simply not conducive to safe, affordable, and high-quality care for patients because of the limits that encumber orthopedic surgeons.
While the AAOS remains convinced that any reforms should protect the rights of a negligently damaged patient to receive just compensation, a decrease in liability costs would improve overall patient care through the reduction of unnecessary spending on often-superfluous defensive medicine. Furthermore, the AAOS is determined that no federal law should supersede any tort reform enacted at the state or local level.
American Academy of Orthopaedic Surgery Hosts Annual Meeting
American Academy of Orthopaedic Surgery
Image: aaos.org
A board-certified orthopedic surgeon in Milwaukee, Wisconsin, Dr. Mark Wichman holds practice affiliation with Aurora Advanced Healthcare Orthopaedics. Dr. Mark Wichman also maintains membership with several professional organizations, including the American Academy of Orthopaedic Surgeons (AAOS).
Established in 1933, the AAOS is a nonprofit organization that offers educational opportunities for orthopedic surgeons and other healthcare professionals. It also advocates for its members and informs the public about this particular field of medicine. In addition, the AAOS awards certification for its members, or fellows.
Each year the AAOS hosts an event where members gather, network, and share ideas pertaining to orthopedic surgery. The 2017 annual meeting, scheduled for March 14 through 18, occurs at the San Diego Convention Center. Typically attracting more than 30,000 guests, the event includes educational sessions where attendees can gain continuing education credit as well as dozens of exhibitors. The gathering also includes an open forum and interactive challenge stations so attendees can participate and ask questions. In addition, for the second year the meeting will feature a Resident Bowl, where residents compete against each other in a trivia game.
